August Taylor in Whats My Grade Again?
Beverly Cosgrove, 5/5/2021, Version 22
What's wrong with Spironolactone? Lots.
Spironolactone ("Spiro") is a potassium-sparing diuretic and steroid drug frequently prescribed in the US to assigned-male-at-nascency (AMAB) trans women as part of their HRT. However, the drug has a number of mild to severe mental side effects, can atomic number 82 to actual changes which most trans women might consider disfiguring, and may interfere with breast development and other feminization.
Spiro began being prescribed to trans women in the early 90's, when the dangers of taking estrogens in the form of Ethinyl Estradiol or Premarin became known. The use of Estradiol solitary, without whatever kind of antiandrogen, is well known to be capable of suppressing testosterone to female levels. (Refs ii,3,4,5) However in the xc's, the Estrogen-related dangers were known to be proportional to dose, and several studies demonstrated an elevated risk of cardiovascular disease within the first i-2 years of HRT initiation. (Ref 6) Studies at the time unfairly lumped all estrogens together, and all progestins together, every bit having the same dangers, a mistake which still lingers today. (7) Equally a result of their unwillingness to treat trans women with high levels of estrogen, Spiro was added to many HRT regimens in the US to assist in suppressing testosterone levels and blocking testosterone effects. Its employ has persisted despite the availability of safe and constructive human-identical estradiol.
Spironolactone does Not feminize significantly, though it is known to encourage some gynecomastia in males. Its sole apply in trans patients is to reduce the upshot of testosterone, and also testosterone levels, a job that estradiol would exercise if a suitable estradiol-only regimen were used instead. Today, AMAB transsexuals often begin their HRT in the U.s. with an "orthodox protocol" consisting of 2-4mg a day of estradiol in pill form plus 200mg a solar day of Spironolactone. Physicians favor this approach because information technology gives a adequately quick reduction in erectile adequacy which can give some fast relief to genitally dysphoric transsexuals.
But there are problems associated with Spiro that your physician may not tell yous about.
Spiro makes information technology more difficult for patients to reach a normal female person hormone balance. There are two furnishings, (1) Inability to reach female level testosterone, and (two) resistance to normal utilization of estradiol. These two effects happen meantime.
The beginning effect is that Spiro doesn't work well in reducing testosterone. A long term written report of New York clinic patients showed that Spiro was unhelpful in achieving basic HRT goals. "Nosotros unexpectedly did not find that Spironolactone aided in testosterone suppression and further establish that it seemed to impair the ability to reach desired serum 17-β estradiol levels." (26) and "Spironolactone did not raise testosterone suppression, and finasteride was associated with college testosterone levels." (28) In another contempo report of patients following a Spironolactone and estradiol protocol, followed for as long as 3.five years showed that the majority did not attain female levels of testosterone in the first couple of years, with only about half attaining information technology past year 3. "Patients with normal BMI started with the highest level of testosterone and demonstrated the steepest turn down between initial visit and 9 months just seemed unable to attain levels of testosterone in the female physiological range overall." Obese patients whose testosterone was already lower than average had somewhat meliorate success with lowering testosterone, merely results were still poor. (23) In the nautical chart below, taken from the same written report, the yellow band shows the female person normal testosterone level. Only later 3 years of treatment did at least one-half of patients fall into that band. Compare this to the profound drop in testosterone acquired past even a single injection of estradiol, in every bit fiddling equally 36 hours. "Suppression of plasma testosterone levels from a hateful of 760 ng/dl… in normal young adult men… to 123 ng/dl was noted 36 h later on estradiol administration."(two) In this sense, a single estradiol injection accomplishes what the Spiro-based protocol may need over three years to do. 
The second effect: taking Spiro, for reasons that are not well understood, appears to interfere with the patient achieving expected blood levels of estradiol. In a contempo study, patients taking Spiro were found to exist unable to achieve expected estradiol levels. "Estradiol levels of patients did not correspond with estradiol dosage administered or BMI. There was no discernable change in serum estradiol levels despite the fact that patients commenced and so continued to take what was believed to be supra-physiologic exogenous estradiol." (23) and "Spironolactone, but non finasteride, utilise was associated with impairment of obtaining desired 17-β estradiol levels." (28)
Spironolactone causes patient cortisol levels to ascent. (Ref one) Patients taking Spiro at doses equally low as 25mg a day experience significantly elevated cortisol levels within a few weeks. (8) However, typical dose for trans women is 200mg per twenty-four hours, despite it being known that doses over 100mg have diminished event. (ix) Normally, the circulating levels of cortisol are tightly controlled past the hypothalamic-pituitary-adrenal (HPA) axis. A fundamental feature of the HPA axis is negative feedback regulation, whereby cortisol suppresses its own secretion. Spiro activates the HPA centrality. However, chronic activation of the HPA axis may play a pathogenic role in a wide range of mutual metabolic and psychiatric disorders, including obesity, depression, and age-associated cognitive dysfunction. (1) In particular, low which does not respond to mutual anti-depressant therapy has been noted in patients with hypercortisolism due to disruption of the HPA centrality, which generally resolves itself once the cause is removed. (xvi,18)
 The effects of Spiro on the brain'due south mineralocorticord system are complex. The primary event as cortisol is raised is a crippling of certain thinking processes, selective attention, visuospatial retentiveness, and mental flexibility/set shifting. In that location is also a modulation, both up and down, of panic and feet and ability to withstand stress. (x) Considering that the time of beginning of a transsexual's hormonal transition may be 1 of the well-nigh stress-inducing periods of the person'due south life, information technology is not surprising that patients receiving Spironolactone complain of "brain fog", poor memory, irritation, anxiety and panic attacks. This also begs the question: could the outset of Spiro-based HRT besides explain increased incidence in the transgender community of self harm, addictive beliefs, and suicide? Data to answer this question is defective, just the adventure seems rational and articulate, and this complex of issues — brain fog, poor retentivity, lethargy, depression, anxiety and panic attack — are widely known in the transgender community. (11) [and Chart (fifteen)] Specially worrying is the evidence that, if a patient is already depressed, adding Spironolactone greatly accelerates the level of hypercortisolism it induces, creating feedback which traps the individual in a depressive state which does not answer to antidepressants. (eighteen)
The effects of Spiro on the brain'due south mineralocorticord system are complex. The primary event as cortisol is raised is a crippling of certain thinking processes, selective attention, visuospatial retentiveness, and mental flexibility/set shifting. In that location is also a modulation, both up and down, of panic and feet and ability to withstand stress. (x) Considering that the time of beginning of a transsexual's hormonal transition may be 1 of the well-nigh stress-inducing periods of the person'due south life, information technology is not surprising that patients receiving Spironolactone complain of "brain fog", poor memory, irritation, anxiety and panic attacks. This also begs the question: could the outset of Spiro-based HRT besides explain increased incidence in the transgender community of self harm, addictive beliefs, and suicide? Data to answer this question is defective, just the adventure seems rational and articulate, and this complex of issues — brain fog, poor retentivity, lethargy, depression, anxiety and panic attack — are widely known in the transgender community. (11) [and Chart (fifteen)] Specially worrying is the evidence that, if a patient is already depressed, adding Spironolactone greatly accelerates the level of hypercortisolism it induces, creating feedback which traps the individual in a depressive state which does not answer to antidepressants. (eighteen)
Just Spiro can actually sabotage the very physical changes that trans women seek through HRT. Increased cortisol is associated with aggregating of visceral fat — hard fatty deposits interlaced with internal organs which causes a swollen abdomen. It is important to discriminate between abdomen adipose fatty, which is soft "jelly similar" fatty direct under the skin, and visceral fatty which is behind the abdominal wall. Visceral fatty requires pregnant effort with diet or exercise to remove and cannot be removed with any kind of ordinary plastic surgery. (20) This visceral fat is caused by raised cortisol. The informal term "Spiro belly" arose because of the perception that those on high doses of Spiro for long term (200mg/day for over a year) seem to often have the characteristic protruding belly. Once visceral fat has accumulated, it is hard to achieve an ideal waist-to-hip size ratio again, even if Spiro is stopped and nutrition and exercise is tried. Research on young girls with poor Waist/hip measurements correlate to college cortisol levels and visceral fat, every bit well as mobilization of fatty from elsewhere in the body to the central region — the opposite of the desired fat mobilization sought by trans women. (12) The clan between hypercortisolism, major depressive illness, and deposits of visceral fatty has been well established. (17)
Finally, Spiro employ is associated with poor chest development in trans women. A preliminary study showed that patients using Spiro instead of another antiandrogen (such as Cyproterone) had significantly more than dissatisfaction with breast development. (13) At this point, the causation is uncertain. The cause could exist the known tendency for Spiro to interfere with the claret levels of estradiol, as verified in multiple studies (23,28). However, information technology is also known that elevated cortisol suppresses Human Growth Hormone, resulting in smaller stature (14) and therefore peradventure, reduced chest growth even in later life. Regardless of the exact explanation, if appears that Trans women are doubly penalized for Spiro use in this respect, considering breast measurement to waist measurement ratio may exist sabotaged at BOTH ends – the very opposite of an "hourglass figure".
If you are taking Spironolactone now, and wish to quit, please be warned — quitting Spiro suddenly without grooming is difficult and hazardous, and your doctor is very unlikely to sympathize some of the problems yous will run across. You should be able to find some peer coaching on the practical aspects of quitting in the Facebook HRT group for more information. Also, experience suggests that well-nigh trans women on megadoses of Spiro (200mg or higher) tin successfully suddenly drib to 100mg a mean solar day without rebound furnishings (speak to your doctor), simply following that, a slower reduction schedule may be required. Only the best solution regarding Spiro is to never start.
Medical specialists and providers have seen the evidence and are finally reconsidering Spiro. A leading Transgender hormone specialist, Dr. Will Powers, has become outspoken in his opposition to the orthodox low-estrogen loftier-Spiro legacy/orthodox treatment protocol. (27) With over 1000 patients in his do, Dr. Powers has established abstention of antiandrogens, especially Spiro, as a key to his "Powers Method". Another key provider with a somewhat similar approach is Dr. Kristen Vierregger. Both these doctors were an influence on, and were probably indirectly influenced by, this very commodity you are reading since its commencement version in 2014.
 Permit me to digress a niggling hither with some commentary. Spironolactone was made function of HRT based on standards ready by The Endocrine Club (19,21) amongst others. By setting a standard for estradiol levels based on 90'due south-era risk data about Premarin and Provera, the nigh dangerous forms of HRT, and ignoring the risk reduction of estradiol 17b given parenterally, they created an artificial standard based on what they did non know rather than what they did know. Only we know much more than now. The risks of injected estradiol levels in the 300-500 pg/ml range are far lower than the risks of suicide or psychotic episodes or sustained mental illness due to mood disturbances from the antiandrogens the prescribers are now offering their patients to keep them below that level. The prescribers are saving their patients from a small adventure by exposing them to a larger risk. It is bad hazard-benefit judgement. I have written more on this elsewhere. (7) It is notable that the 2009 version of The Endocrine Society guidelines fifty-fifty include a mention of estradiol injection (19) but still refer to Spironolactone. One last thought, this time a speculation: it seems possible based on observations that high levels of testosterone provide some protection against the cortisol-raising backdrop of Spironolactone, such that testing of the drug on male volunteers might not have shown such a large side consequence when the drug was originally tested, leading to a situation where heavy dosing of trans women led to these oversized furnishings. Would the original manufacturer'due south dosing advice have been different if the drug had been more thoroughly tested with female patients? Something worth looking into, mayhap.
Permit me to digress a niggling hither with some commentary. Spironolactone was made function of HRT based on standards ready by The Endocrine Club (19,21) amongst others. By setting a standard for estradiol levels based on 90'due south-era risk data about Premarin and Provera, the nigh dangerous forms of HRT, and ignoring the risk reduction of estradiol 17b given parenterally, they created an artificial standard based on what they did non know rather than what they did know. Only we know much more than now. The risks of injected estradiol levels in the 300-500 pg/ml range are far lower than the risks of suicide or psychotic episodes or sustained mental illness due to mood disturbances from the antiandrogens the prescribers are now offering their patients to keep them below that level. The prescribers are saving their patients from a small adventure by exposing them to a larger risk. It is bad hazard-benefit judgement. I have written more on this elsewhere. (7) It is notable that the 2009 version of The Endocrine Society guidelines fifty-fifty include a mention of estradiol injection (19) but still refer to Spironolactone. One last thought, this time a speculation: it seems possible based on observations that high levels of testosterone provide some protection against the cortisol-raising backdrop of Spironolactone, such that testing of the drug on male volunteers might not have shown such a large side consequence when the drug was originally tested, leading to a situation where heavy dosing of trans women led to these oversized furnishings. Would the original manufacturer'due south dosing advice have been different if the drug had been more thoroughly tested with female patients? Something worth looking into, mayhap.
The medical community owes it to the transsexual community to take a second wait at the overall hazard/do good ratio for the use of Spironolactone as an antiandrogen. Not only is in that location testify that Spiro may be interfering with the primary goal of HRT, but Spiro may exist directly responsible for patient damage by crippling the cognitive ability of patients and compromising their ability to withstand stress — a terrible burden for this highly stressed minority.
SOME ANECDOTAL EXPERIENCES
—
"The curt term memory deficit and cognitive impairment were debilitating side effects of 25mg over a month's time. This along with unusual bruising,dizziness/unsteadiness, and chronic burnout prompted me to stop taking information technology. I can't imagine what might take happened with the mutual higher doses.", MT, December 2016
—
"Was on that crap for 21 months. Lowered information technology from 200mg/day to 100, then 50, then 0. This was in Oct. of this year. Since so all the symptoms are going away. I also stopped using finasteride. Switched from pills and oral P4 to injectable EV and P4. 5mg EV and 20mg P4 every iii.five days. Feeling much better.", KA, Dec 2016.
—
"After taking it for about iv years it started to just quit blocking T all together. I was on injected estradiol valerate and withal my T was at 400! Believe me that Spiro is bad shit. Information technology cost me my job. The brain fog and short term memory loss may exist permanent. Depression was increased and not to mention the long term memory I lost.", SL, Dec 2016.
—
"I had a lot of emotive/cognitive bug with Spiro that noticeably improved when I dropped information technology after two years (my high E2 level allowed this)." BRB, Dec 2016.
—
"I had a bout of severe dizziness and got a very itchy rash which my housemates initially thought was a problems bite then later on confirmed information technology was not similar any bug bite they'd ever seen. The rash grew larger and more itchy over the course of a week, it disappeared completely a twenty-four hour period or two after I stopped taking Spiro. While on Spiro I experienced greater difficulty with organizing thought, more frequent thought derailment, and more than reactionary and unclear thinking. These severely impacted my job operation every bit I rely heavily on memorized diagnostic procedures to solve calculator issues. The mental side effects of Spiro dissipated rapidly for me after I stopped taking it.", RM, Dec 2016.
—
"I personally can't stand up Spiro! Been on it since May…tomorrow is 7 months. I've had severe side furnishings since the beginning. Here is my list: tired, retentiveness loss, brain fog, light headed, anxiety, poor breast development, severe depression, constipation, dehydration, and low blood pressure. I've been a mess since the beginning. I take the pill form. Looking into asking my doctor about moving over to injections and switching to progesterone and keeping my estradiol going.", JMS, Dec 2016.
—
"I was on it for 6 months at a low dose, stopped taking and upped my. Estridol and progesterone. I don't and didn't want to showtime down the road. Had the mental side furnishings.", DBS, December 2016.
—
"my endo started me on 200mg spiro daily with estradiol and i started getting spells of difficulty breathing, debilitating migraines (which i have never experienced before/non a headachey person), increased feet, fatigue, yadda yadda. she actually didnt recall information technology was the spiro (and theres not too much info about spiro online??) but nosotros cut it out and i cant begin to tell you lot how much better i feel" DS, 1-5-18
—
"Started on Estradiol and Spiro pills… Wasn't getting anywhere with my E and T levels. After 6 months, switched to EV injections and dropped the Spiro, considering of this forum. Now I'thousand consistently in ideal range of Due east and T. Information technology'south very possible with no Spiro.", AA, ane-v-18
—
"I switched from spiro to cypro just a few days ago. Ok, its still an AA, but its the lesser of two evils equally Beverly pointed out in a previous thread when I asked. In that few days, the brain fog has already gone, I accept elevated energy levels and i'm not feeling tired constantly. I no longer pee like a race horse. Getting off spiro will just do good your wellness. If my E levels are right next calendar week when I get for my bloods, i'll be dropping the cypro too." EC, 1-v-18
—
"I have a bad reaction to antiandrogens. I'm now completely off of spironolactone, feminizing rapidly, experience very healthy, and have no encephalon fog or other symptoms typical to longer term exposure to anti androgens. I'm just taking injectable estradiol valerate at a normal dosage, subcutaneous twice a week to keep levels more stable, and micronized progesterone. I am pre-op and my testosterone is actually lower than the female alphabetize range without antiandrogens.", JM, 1-6-2017
—
"I dropped 200mg of daily Spiro. Increased my Eastward from 4mg to 8mg. My E increased and T dropped and got my libido back. Worked for me. In 2 weeks at next DR. appt, I am going to ask to switch from pills to injections.", SK, 8-1-2018.
—
"I besides experience 1000 times better since dropping Spiro and taking no AAs, I like the E and p only for T suppression, works fashion better that I had always expected, almost too skilful actually.", RS, 1-eight-2018.
—
"I was but on it about 1.five months and already had bad brain fog and perchance other developing problems. I THINK am in the clear for whatsoever permanent negative effects from it, just I worry.", NK, 6-one-2020.
—
"I hate Spiro and only took it for a couple of months. It acquired precipitous pains in my muscles, and too caused deep depression. I will never accept it again. There are several alternatives to Spiro. Another I will not take is Finasteride, due to it's side effects.", AT, 5-27-2020.
—
"I was on both low Eastward doses and high spiro. Thought I was done with my programming career. At present I'm on EV, progesterone and no blockers. My brain is back." One thousand.Fifty., 4-xxx-2021
—
"I'm a lot better since dumping spiro. I started to calm downward upon starting East, but brain fog got worse – not to mention I was constantly dehydrated. Estrogen – WITHOUT spiro – has vastly improved the cerebral issues I had in the 10 years prior to HRT, killed the rhoid rages, and continues to heal the depression and other emotional issues I had had since starting puberty.", J.D., 4-30-2021
REFERENCES and LINKS
(1) "Combined Receptor Antagonist Stimulation of the Hypothalamic-Pituitary-Adrenal Axis Test Identifies Impaired Negative Feedback Sensitivity to Cortisol in Obese Men", Mattsson C, The Periodical of Clinical Endocrinology & Metabolism, Book 94, Issue iv, 1 Apr 2009, Pages 1347–1352, https://doi.org/10.1210/jc.2008-2054
(2) " Direct inhibition of Leydig jail cell function by estradiol.", Jones TM, J Clin Endocrinol Metab. 1978 Dec;47(6):1368-73.
(3) " The result of oestrogen administration on plasma testosterone, FSH and LH levels in patients with Klinefelter's syndrome and normal men." Smals AG, Acta Endocrinol (Copenh). 1974 Dec;77(4):765-83.
(4) "In men, peripheral estradiol levels straight reflect the activeness of estrogens at the hypothalamo-pituitary level to inhibit gonadotropin secretion.", Raven G, J Clin Endocrinol Metab. 2006 Sep;91(9):3324-eight. Epub 2006 Jun 20.
(5) "Sex steroid control of gonadotropin secretion in the man male. Two. Furnishings of estradiol administration in normal and gonadotropin-releasing hormone-deficient men.", Finkelstein JS, J Clin Endocrinol Metab. 1991 Sep;73(three):621-8.
(6) "Hormone Therapy Dose, Conception, Road of Delivery, and Hazard of Cardiovascular Events in Women: Findings from the WHI Observational Study", Shufelt C, Menopause. 2014 Mar; 21(3): 260–266.
(7) "What Went Wrong With MTF Hormonal Therapy?", Cosgrove, B.
(8) "Effect of eplerenone versus spironolactone on cortisol and hemoglobin A₁(c) levels in patients with chronic eye failure", Yamaji One thousand, Am Heart J. 2010 November;160(5):915-21
(9) "Spironolactone Dose-Response Relationships in Salubrious Subjects", McInness Thousand, Br. J. clin. Pharmac. (1982), 13, 513-518
(10) "Blockade of the Mineralocorticoid Receptor in Good for you Men: Effects on Experimentally Induced Panic Symptoms, Stress Hormones, and Noesis", Otte C, Neuropsychopharmacology (2007) 32, 232–238
(11) "Hormone Therapy is Lifesaving — But Why is No One Studying Its Long-Term Effects?", Out Magazine, Tourjee D, 2016-09-20 09:38
(12) "Stress and Intestinal Fat: Preliminary Evidence of Moderation by the Cortisol Awakening Response in Hispanic Peripubertal Girls", Donoho C, Obesity (2011) nineteen, 946–952
(13) "Predictive Markers for Mammoplasty and a Comparison of Side Effect Profiles in Transwomen Taking Various Hormonal Regimens", Seal LJ, The Periodical of Clinical Endocrinology & Metabolism, Volume 97, Issue 12, ane Dec 2012, Pages 4422–4428
(14) "Cortisol and growth hormone: clinical implications of a complex, dynamic relationship", Stratakis CA, Pediatr Endocrinol Rev. 2006 Apr;iii Suppl 2:333-8.
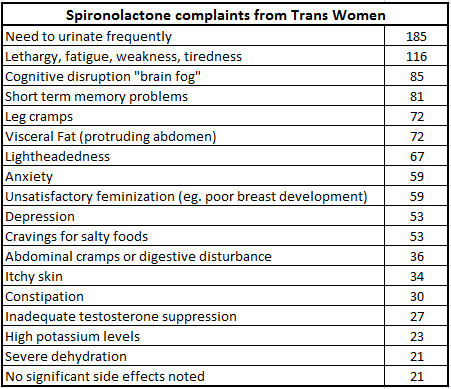
(15) Chart from agile survey of over 200 Spironolactone patients, from Online Facebook Group, "The MTF Trans HRT Hormone Forum", founded Dec. 2014, membership approx 9800.
(16) "Handbook of Stress and the Brain: Stress: integrative and clinical aspects", Elsevier. pp. 440–
(17) "Increased Intra-Abdominal Fatty Degradation in Patients with Major Depressive Illness as Measured by Computed Tomography", Thakore J, BIOL PSYCHIATRY 1997;41:1140-1142
(18) "Mineralocorticoid receptor function in major depression", Young EA, Arch Gen Psychiatry. 2003 January;60(ane):24-8.
(19) "Endocrine Treatment of Transsexual Persons:An Endocrine Guild Clinical Exercise Guideline", Hembree W, The Journal of Clinical Endocrinology & Metabolism, Volume 94, Outcome ix, 1 September 2009, Pages 3132–3154
(xx) "High visceral fat mass and high liver fatty are associated with resistance to lifestyle intervention.", Thamer C, Obesity (Silver Spring). 2007 Feb;fifteen(2):531-8.
(21) "Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Guild Clinical Practice Guideline", Hembree WC, The Journal of Clinical Endocrinology & Metabolism, Volume 102, Issue 11, i November 2017, Pages 3869–3903
(22) "The 45-twelvemonth story of the development of an anti-aldosterone
more specific than spironolactone", Menard J, Molecular and Cellular Endocrinology 217 (2004) 45–52
(23) "Testosterone Levels Achieved by Medically Treated Transgender Women in a United States Endocrinology Clinic Cohort", Liang J, Endocrine Do: February 2018, Vol. 24, No. ii, pp. 135-142.
(24) "The issue of oestrogen administration on plasma testosterone, FSH and LH levels in patients with Klinefelter's syndrome and normal men." Smals AG, Acta Endocrinol (Copenh). 1974 Dec;77(iv):765-83.
(26) "Hormonal Treatment of Transgender Women with Oral Estradiol", Leinung Grand., https://doi.org/x.1089/trgh.2017.0035
(27) Dr. Will Powers, Video lecture, "Anti-Androgens and Spironolactone issues in MTF HRT | Dr Will Powers @ OUWB" Youtube link: https://youtu.be/LX8AdkL7u0s
(28) Leinung K.C., Feustel P.J., Joseph J. Hormonal treatment of transgender women with oral estradiol. Transgend. Wellness. 2018;3:74–81. doi: 10.1089/trgh.2017.0035.[PubMed]
sullivanseepince1950.blogspot.com
Source: https://moderntranshormones.com/2018/01/01/whats-wrong-with-spironolactone/
0 Response to "August Taylor in Whats My Grade Again?"
إرسال تعليق